Recovering from a major injury or surgery takes a lot of commitment, dedication, and grit. As physical therapists, athletic trainers, and medical providers, it can be challenging to find ways to motivate, encourage, and demonstrate progress to your patients when recovery is measured over many months or even years.
In today’s blog post, we take you all the way through a patient case study that highlights the implementation and efficacy of surface EMG biofeedback during rehabilitation. We will take a deeper look into how the specific features of the mTrigger device can be leveraged to improve outcomes, track changes, and encourage progress.
Patient Overview
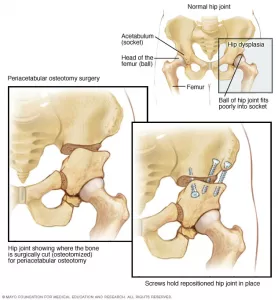 Our patient is a 32-year-old female s/p right hip labral reconstruction and periacetabular osteotomy (PAO). This former collegiate athlete had a 20-year history of bilateral hip pain stemming from a very lo
Our patient is a 32-year-old female s/p right hip labral reconstruction and periacetabular osteotomy (PAO). This former collegiate athlete had a 20-year history of bilateral hip pain stemming from a very lo
ng and successful career as a competitive gymnast. After years of hip pain and failed surgeries, she elected to undergo bilateral hip labral reconstructions and PAO (not at the same time) for hip dysplasia.
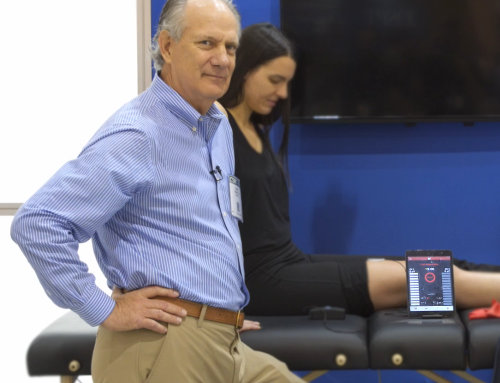
We started using mTrigger biofeedback right away, just a few days after surgery. Since the surgery requires a spinal block with a subsequent pain catheter, full muscle function is not recovered for several days following the surgery. In this video, the effects of the anesthesia are still wearing off and the patient does not yet have full volitional muscle control of the glutes. We started with a simple glute squeeze to assess the level of muscle activation available and begin the process of re-establishing neuromuscular control.
Typically, during a labral reconstruction with PAO, the patient is partial weight bearing for 8-16+ weeks (14 weeks in this case). Thus, progress is slow and being able to track incremental changes is imperative. Early on, we targeted the leg and hip muscles in non-weight bearing or partial weight bearing positions that did not stress the surgical repair and osteotomy.
Over the course of the next several months, we really honed-in on tracking the progress of three major muscle groups and their functional patterns: quads, glutes, and hamstrings.
Quads and Squats
To start out, we began assessing the strength and activation level of the quadricep muscles in a non-weight bearing position. Simple exercises like quad sets, long and short arc quads were utilized to keep the legs moving and muscle activation primed for the next phase of rehab. Straight leg raises (although a great exercises for a lot of cases) were avoided here due to the excessive strain they place on the hip flexors and anterior joint capsule.
The neuro muscular deficit function was used once a sufficient muscle contraction and safe movement pattern was achieved to 1) test out the existing deficit 2) provide a starting point and 3) track process over the coming weeks.
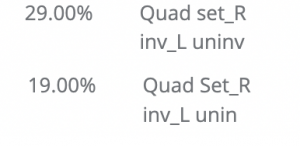
Here is a glimpse of how quad function improved over time.
From week 9 to week 12 post op, a simple quad set NMDT improved from 29% to 19%.
At week 11, while the patient was partial weightbearing (50-75%) we performed a NMDT using a body weight mini squat to access the deficit in a more functional position. As you would expect, the deficit was greater than in NWB, but not far off.
![]()
Throughout the next several weeks, mTrigger biofeedback was used to help with improving squat form, weight shift, and equal loading capacity through the hip joint. We started with body weight and a tolerable range of motion, then progressed from there. In the left hand column, we see the average MVC on the left side (CH 1) and in the right column you see average MVC on the right side (CH 2) during the exercise.
Week 10 Body Weight TRX Squats (Column 1 – left/Column 2 – right)
![]()
Week 12 Body Weight/Light Weight Squats (Column 1 – left/Column 2 – right)
![]()
Week 17 Squats 20lbs (Column 1 – left/Column 2 – right) ![]()
Notice how the activation of the quad continues to increase steadily over each week. With added weight we can expect to see one of two things: either an increase in muscle activation to match the increased demand of the exercise, OR a greater weight shift off the involved side because it is not able to meet the new demand. In this case, we see an increase in activation of in the involved side, which is great!
Once the patient began walking normally, we started to incorporate single leg exercises into her training program. Initially, TRX straps were used to help offload some weight during a right leg lunge. Here are the results.
Week 12- TRX R Lunge (Column 1 – right)
![]()
Over the next several weeks, the patient was able to tolerate regular lunges and lunge progressions.
Week 13- R Lunge (Column 1 – right)
![]()
Notice the decrease in quad activation with increased WB. In this case, instead of increasing muscular activation to meet a higher exercise demand, the patient shifted more weight into the back leg due to pain and weakness. However, with the following weeks we see excellent progress with improved movement patterns and quad activation.
Week 17- R lunge (Column 1 – right)
![]()
Around this time, lunging variations were also added to help challenge the hip in different planes. We used mTrigger biofeedback bilaterally in order to compare activation levels from right to left side.
Left Lateral Lunge (Column 1 – left) – uninvolved
![]()
Right Lateral Lunge (Column 1 – right) – involved
![]()
A lower activation level on the surgical right side, which isn’t surprising for the first time, but overall, not bad at all.
In the second half of this case study, we will dive deeper into the involvement and recovery of the hamstrings and the ever-important hip stabilizers. The Glutes.
CHECK OUT OUR DOWNLOADABLE 3-PHASE POST-OP HIP PROTOCOL HERE!
When to Use Biofeedback in Treatment
|
More Uses for Biofeedback
|
Image: https://www.mayoclinic.org/diseases-conditions/hip-dysplasia/multimedia/img-20126290





Leave A Comment